Achilles tendon healing after a rupture is a biological process that takes months, not days. Your body moves through three overlapping phases — inflammation, then a proliferative “bridge-building” stage, then remodelling — and the middle stage is when the new tissue is easiest to overstretch. Understanding that timeline helps you see why boot angle, wedge removal, and night protection are not bureaucracy; they are guardrails while your tendon finds its length.
Contents
- Key Takeaways
- The Three Phases of Tendon Healing
- Why the “Bridge” Weeks Matter
- Protected Movement vs Risky Movement
- What Research Says About Tendon Length
- What This Means for Your Recovery
- Frequently Asked Questions
- References
Key Takeaways
- Achilles tendon healing after rupture follows three phases: inflammatory, proliferative (new collagen bridges the gap), then remodelling and strengthening
- Weeks 3–6 are often described as the proliferative phase — new tissue is present but still fragile
- Unprotected dorsiflexion (pulling the toes up), forcing stretches, or speeding up wedge removal can encourage the tendon to heal in a longer, slacker position (tendon elongation)
- Protected early weight-bearing in your walking boot is not the same as loading the tendon in a flat foot or bare ankle — many protocols encourage safe walking inside the rules your team sets
- Compliance beats gadgets: whichever boot you wear, following angle and progression schedules matters more than the brand name
- If something feels wrong after a slip or stretch — new pop, sharp change in symptoms — seek urgent medical review
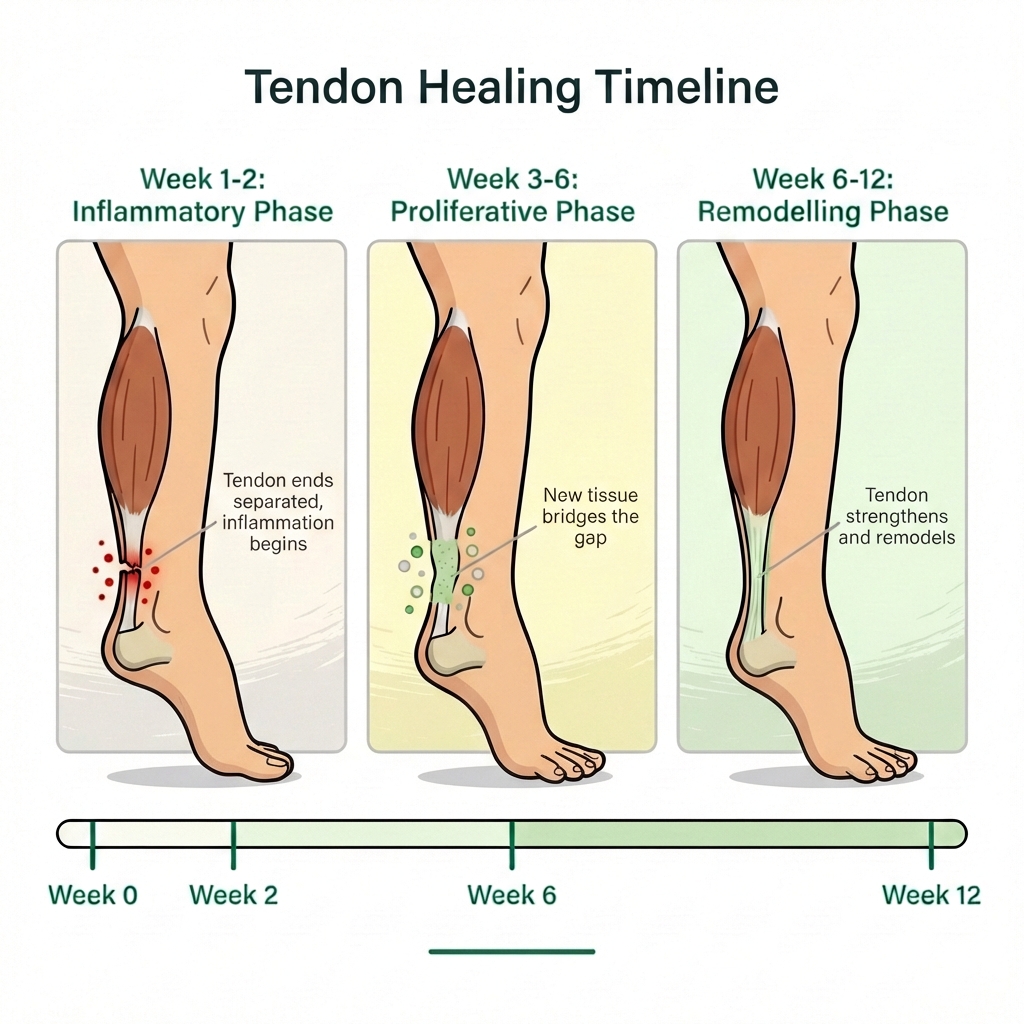
The Three Phases of Tendon Healing
The infographic at the top of this article summarises the same story clinicians use when they talk about tendon healing biology. Timings vary slightly between people and protocols, but the pattern is consistent:
| Phase | Typical period* | What is happening | Patient-friendly picture |
|---|---|---|---|
| Inflammatory | ~weeks 1–2 | Bleeding and inflammation settle; cells arrive to start repair | The “cleanup and alarm” phase after the tear |
| Proliferative | ~weeks 3–6 | New collagen and blood vessels bridge the gap | A fragile scaffold between the ends |
| Remodelling | ~weeks 6–12 and beyond | Collagen reorganises, stiffens, and aligns with load | The scaffold matures toward stronger tendon |
*Weeks are approximate; your clinician’s protocol is the one that counts.
For a broader week-by-week view of appointments, boots, and milestones, see our Achilles rupture recovery timeline. Phase-specific guides such as weeks 4–6 sit in the same recovery pathway.
Why the “Bridge” Weeks Matter
During the proliferative phase, the new tissue is nothing like your original Achilles yet. It can carry some load in a protected position, but it tolerates poorly being stretched while immature.
That is the idea behind warnings about tendon elongation — sometimes described as healing “long.” The torn ends can still unite, but if the gap is held open repeatedly by early dorsiflexion or progressing angles too fast, the repair may lengthen. Longer tendons can make it harder for the calf to generate power, though human outcomes are not as simple as a single ultrasound number (see below).
This is also why night protection matters: rolling over in bed with the foot flopping up is a classic way to stress a fresh repair. If the boot is unbearable overnight, discuss options with your team — many patients use a purpose-built night splint designed for safe sleeping positions.
Protected Movement vs Risky Movement
Modern Achilles care often includes early weight-bearing as tolerated — but protected by a boot (and sometimes crutches) and always within the angle your protocol allows. That is different from:
- Standing or walking without the boot
- Removing heel wedges early because you “feel ready”
- Pushing the ankle upward to “stretch the calf”
- Long steps or hills that force dorsiflexion inside the boot beyond your allowed range
Physiotherapy often starts in the week 3–6 window, but early sessions focus on safe loading, hip and knee control, and circulation — not aggressive stretching. If you want a structured, patient-friendly walkthrough of expectations and exercises, our Achilles recovery course follows the same principles: gradual progression, no shortcuts.
What Research Says About Tendon Length
Imaging studies after Achilles rupture often report measurable tendon elongation — one systematic review found mean lengthening on imaging from about 0.15 cm to 3.1 cm across studies, with mixed links to symptoms and strength tests in the general population. Biomechanical work more often shows an effect of elongation on how the tendon behaves under load, even when day-to-day scores still look acceptable.
Prospective work on early functional mobilisation after surgical repair shows that how loading is introduced over time affects tendon length and calf muscle size — a reminder that gradual, protocol-led progression is not the opposite of movement; it is controlled movement.
None of this means you should be frightened of every step in the boot. It means the rules exist to keep dorsiflexion and load inside what that week’s tissue can handle.
What This Means for Your Recovery
- Treat wedge or hinge changes like medication doses — do not skip ahead because you feel good one day.
- Keep the boot on whenever you are upright or at risk of tripping; plan showering and sleep with your team’s advice.
- Walk as allowed in the boot to help calf pump activity and general fitness; if you were prescribed blood thinners, staying mobile (within instructions) also supports vein health.
- Ask before “testing” the ankle — a single unprotected forced stretch is not worth the experiment.
- Use rehab for strength and control, not to “speed up” biology you cannot see.
If your hospital’s leaflet disagrees slightly with this article, follow your own team — protocols differ by country, surgeon, and whether you had surgery.
Frequently Asked Questions
What is the proliferative phase of Achilles healing?
Roughly weeks 3–6 after rupture, your body lays down new collagen that bridges the gap between torn tendon ends. That tissue is weaker than normal tendon and easier to stretch out if the ankle is pulled upward (dorsiflexion) without protection or if you advance your boot angle too fast.
Can I walk during the proliferative phase?
In most modern protocols, yes — but in your boot, with crutches only if your team told you to use them, and only as much as your protocol allows. Early weight-bearing in a protected position is different from standing barefoot, stretching your calf, or removing wedges early. If you are unsure, ask your clinician before changing anything.
Does tendon elongation always ruin my outcome?
Not necessarily. Imaging studies often show some lengthening after Achilles rupture, and the relationship to how you feel day-to-day is complex. Some people function very well even with measurable elongation. That said, protecting length while the new tissue is forming is still sensible — it stacks the odds in your favour for calf power and push-off later.
What are the signs I may have damaged healing tissue?
A new pop or snap, sudden loss of confidence in the repair, a sharp change in gap or position (if you were told you had a large gap), or a big increase in pain after a specific incident should trigger urgent contact with your fracture clinic or A&E. When in doubt, get checked — re-rupture is uncommon overall (roughly 3–5%) but serious.
When can I start physiotherapy?
Many teams begin supervised rehabilitation around weeks 3–6, but the exercises are controlled and respect your boot angle — not aggressive stretching. Follow your own programme: aggressive stretching too early is not recommended until the tendon is well healed (often 12–18 months for hard stretching goals).
References
-
Diniz LO, Pacheco FS, Guerra-Pinto F, Pereira BS, Ferreira A, Kerkhoffs GMMJ. Achilles tendon elongation after acute rupture: is it a problem? A systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(12):3982-3991. DOI: 10.1007/s00167-020-06010-8
-
Aufwerber S, Edman G, Grävare Silbernagel K, Ackermann PW. Changes in Tendon Elongation and Muscle Atrophy Over Time After Achilles Tendon Rupture Repair: A Prospective Cohort Study on the Effects of Early Functional Mobilization. Am J Sports Med. 2020;48(13):3296-3305. DOI: 10.1177/0363546520956677
-
Tarantino D, Palermi S, Sirico F, Corrado B. Achilles Tendon Rupture: Mechanisms of Injury, Principles of Rehabilitation and Return to Play. J Funct Morphol Kinesiol. 2020;5(4):95. DOI: 10.3390/jfmk5040095 (PMC free article)
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1564-1571. DOI: 10.1177/0363546512447926
Primary source: Diniz LO, Pacheco FS, Guerra-Pinto F, et al. (2020). Achilles tendon elongation after acute rupture: is it a problem? A systematic review
