Stage 2 Achilles rehab is where many people hit their first “double challenge”: your ankle feels stiff, but your tendon is still healing.
That is why Stage 2 is not a sprint to full flexibility. It is a balance between:
- Restoring ankle mobility (range you can move comfortably through)
- Protecting tendon integrity (avoid excessive dorsiflexion and strain before your capacity is ready)
In practice, this means controlled and low-risk exercise selection. Two common components are:
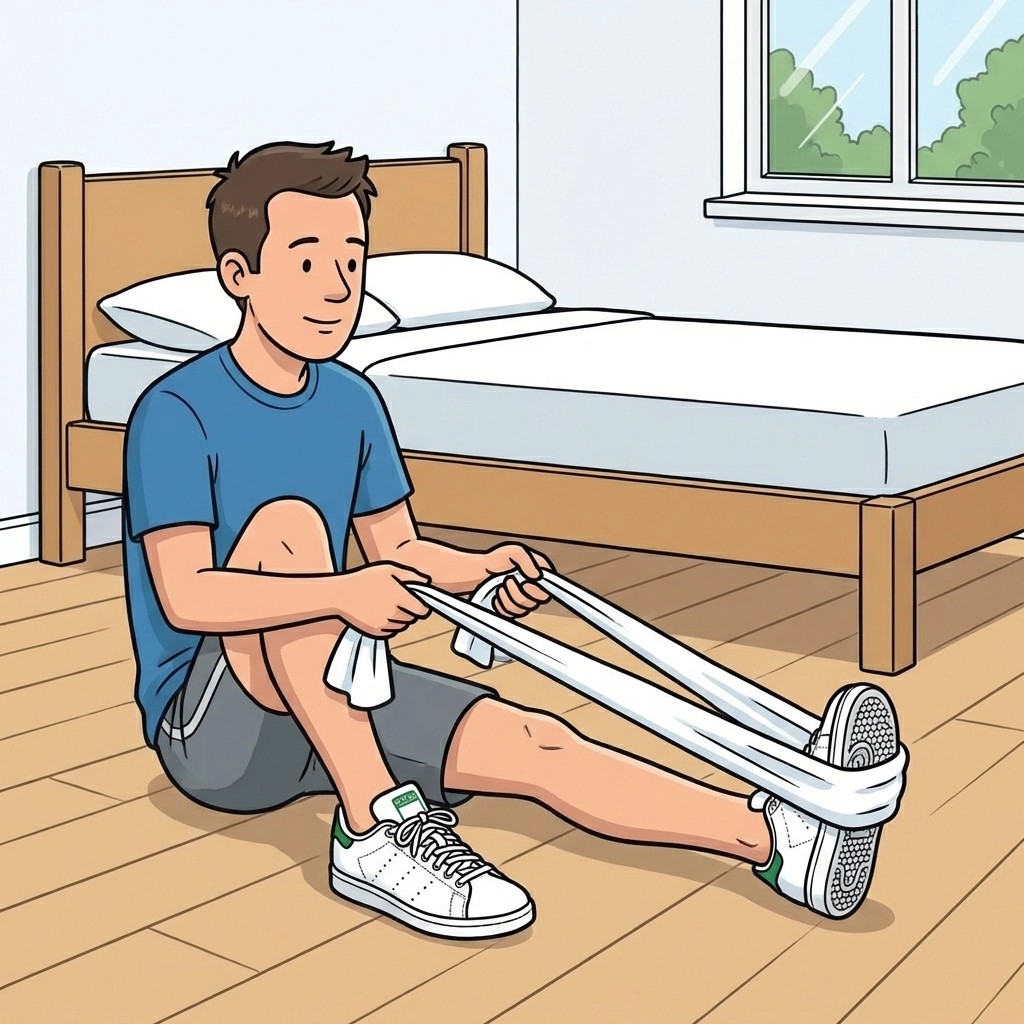
- Gentle mobility work (for example, towel stretch)
- Resistance band loading (controlled plantarflexion against gentle resistance)
The core rule is restraint. Early overcorrection with aggressive stretching may increase the risk of the tendon healing “long” or becoming mechanically less efficient. Instead, prioritize controlled loading first, then gradually widen your range.
Contents
- Why Stage 2 needs restraint (mobility + tendon loading)
- Gentle mobility: what “safe stretch” looks like
- Resistance band plantarflexion: why load comes before maximal range
- Mobility vs load: the practical difference
- How to monitor symptoms and progress safely
- What this means for your recovery
- Frequently asked questions
- References
Why Stage 2 needs restraint (mobility + tendon loading)
After immobilisation, stiffness is expected. But your body is not just “tight”; your tendon-calf unit also needs time to regain length-tension balance and tendon stiffness for normal gait.
If you push range aggressively before strength and control catch up, you can expose the tendon to more strain than it is ready for. That is why many modern protocols aim for early, functional rehabilitation that combines weight-bearing and targeted exercises rather than end-range stretching alone (Zellers and colleagues, 2019).
A key concept: function beats flexibility
The goal is not “how quickly can I stretch.” The goal is: restore walking function without compromising tendon integrity.
Gentle mobility: what “safe stretch” looks like
Gentle mobility work is useful when it:
- Feels like a mild stretch, not a painful stretch
- Is symptom-guided (you do not spike pain during or after)
- Does not leave you more stiff or limping the next day
- Does not turn into a “force it further” contest
Practical examples (keep them gentle):
- Towel stretch held comfortably without forcing end range
- Calf mobility in a range that does not increase irritability
Avoid in early Stage 2:
- Forced dorsiflexion “to the point of sharp discomfort”
- Aggressive stretching that leaves you sore/swollen later
- Stretching as the main training stimulus while load tolerance is still building
For wider context on boot-to-shoes progression and when range increases, see walking boot removal timing and boot wedge removal protocol.
Resistance band plantarflexion: why load comes before maximal range
Loading the calf-tendon unit helps restore stiffness and muscle activation in a controlled way.
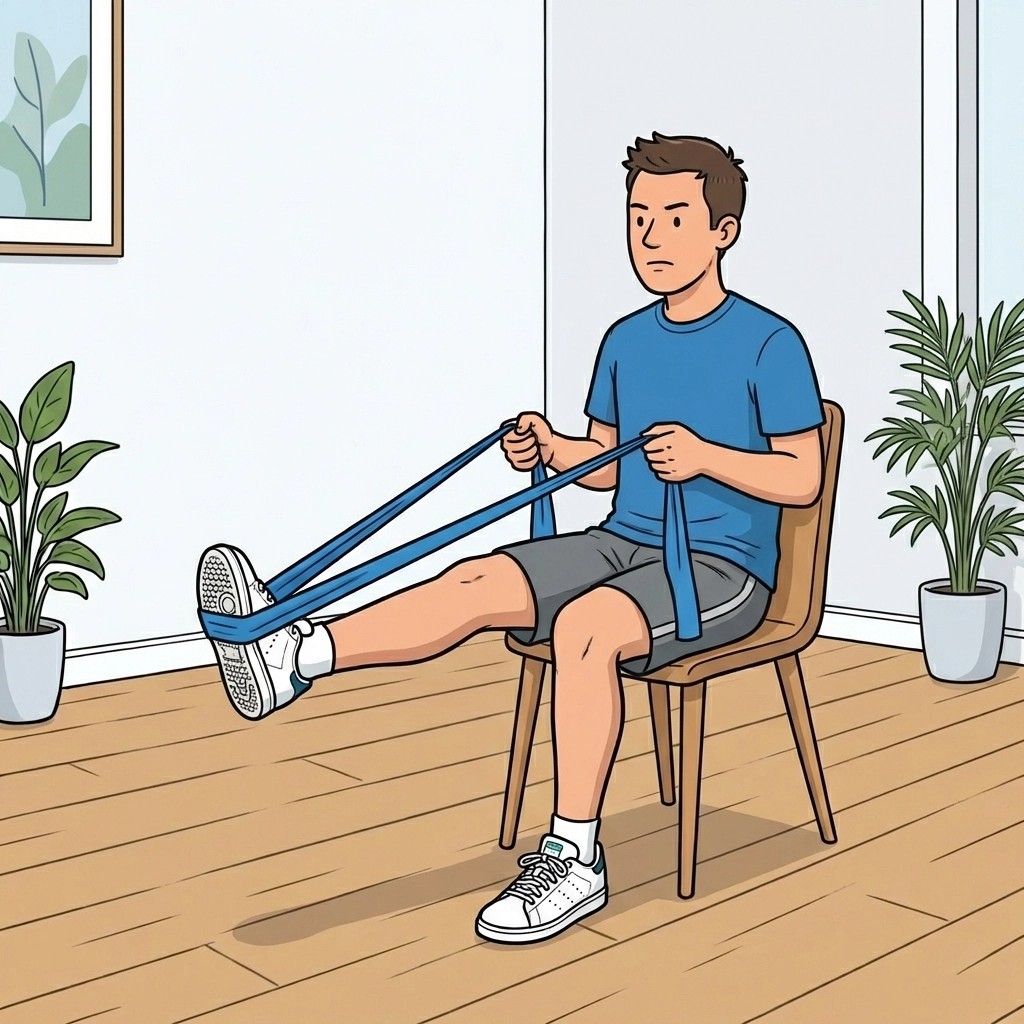
When you use a resistance band for plantarflexion, you are:
- Training plantarflexor strength gradually
- Introducing tendon load through a controlled movement path
- Progressing capacity before you chase maximal dorsiflexion range
How to keep band work tendon-safe:
- Start with light resistance
- Use a slow tempo
- Keep ankle alignment controlled (avoid rolling the ankle out)
- Stop if you get sharp pain, a “giving way” sensation, or next-day flare
This principle matches how we frame rehab more broadly on the site: strength and loading progression come first, with stretch and range added carefully afterward.
Mobility vs load: the practical difference
| Component | What it should do | What it should not do |
|---|---|---|
| Gentle mobility (towel stretch) | Restore comfortable ankle range | Force end-range dorsiflexion or cause symptom spikes |
| Resistance band plantarflexion | Build tendon stiffness and load tolerance | Overload too fast, with messy form or next-day flare |
If you are unsure which direction your exercise response points, use a simple guide:
- Better next day = you are likely in the right dose range.
- Worse next day (more swelling, more limp, worse pain) = reduce intensity and consult your physio.
How to monitor symptoms and progress safely
During Stage 2, the tendon-calf unit is still “learning” how to handle increased demands. Progression is safest when you track:
- Next-day swelling and stiffness
- Change in gait (does push-off feel worse, does limp increase?)
- Heel-rise quality if you are already testing it in your programme
- Pain response curve (not just during exercise, but over 24 hours)
If symptoms worsen, do not “push through.” De-load and review with your clinician.
What this means for your recovery
Do:
- Use gentle, symptom-guided mobility to restore range comfortably
- Use controlled plantarflexion loading (often with resistance bands early in Stage 2)
- Progress based on response, not only time
Avoid:
- Forced stretching in early phases
- Turning mobility work into the main driver of training when your capacity is still rebuilding
In plain language: regain function without compromising tendon integrity.
Frequently asked questions
Can I do towel stretching after Achilles rupture in Stage 2?
Yes, if it is gentle and symptom-guided. Avoid forced end-range dorsiflexion.
Why is aggressive stretching discouraged early?
Because the healing tendon-calf unit can be vulnerable to increased strain before capacity is rebuilt.
When should I start resistance band plantarflexion?
Usually early Stage 2 once your clinician progresses you beyond strict protection. Start low and progress slowly.
What guides progression best?
Symptoms and movement quality, especially next-day response.
Can I regain ankle motion and still protect my tendon?
Yes. The strategy is restraint: gentle range plus controlled loading.
References
-
Zellers JA, Carmont MR, Grävare Silbernagel K. Defining Components of Early Functional Rehabilitation for Acute Achilles Tendon Rupture: A Systematic Review. Orthop J Sports Med. 2019;7(11):2325967119884071. https://doi.org/10.1177/2325967119884071
-
Silbernagel KG, Steele R, Manal K. Deficits in Heel-Rise Height and Achilles Tendon Elongation Occur in Patients Recovering from an Achilles Tendon Rupture. Am J Sports Med. 2012;40(7):1568-1575. https://doi.org/10.1177/0363546512447926
-
Maquirriain J. Achilles Tendon Rupture: Avoiding Tendon Lengthening during Surgical Repair and Rehabilitation. Yale J Biol Med. 2011;84(3):289-300. (PMC3178860)
-
Okoroha K, et al. Comparison of Tendon Lengthening with Traditional vs. Accelerated Rehabilitation After Achilles Tendon Repair: A Randomized Controlled Trial. Orthop J Sports Med. 2019;7(7 suppl5):2325967119S00323. https://doi.org/10.1177/2325967119S00323
Primary source: Zellers JA, Carmont MR, Grävare Silbernagel K. Defining Components of Early Functional Rehabilitation for Acute Achilles Tendon Rupture: A Systematic Review
